31 May World class African – European AIGHD-led consortium joins forces for revolutionary health technology to fight pediatric mortality
Every year, more than two million children in low-resource settings die due to substandard quality of care caused by constraints in healthcare systems. Shortage of staff and lack of adequate equipment lead to millions of children dying from conditions that are treatable at low costs.
It was these glaring curable conditions that frustrated Dr. Job Calis in his recurring visits to Malawi throughout his career and inspired him to look for solutions. After working in Malawi as both a PhD student and in the pediatric intensive care unit treating children with diseases, Job wanted to make a difference on a larger scale. “I was hoping to make a big impact with the paediatric intensive care unit by reducing child mortality in the hospital, which is around 3 to 5%, but I realized that most of the kids didn’t make it to my unit in time, and I was not making as big of an impact as I had hoped.”
This dissatisfaction would inspire Dr. Job Calis to return to Malawi for an initiative utilizing cutting edge technology to resolve child mortality: Project IMPALA. Essentially, this is a monitoring system utilizing a series of innovations to curb child mortality in African hospitals, from the use of artificial intelligence to detect and predict health complications, to contactless sensors embedded in a mat, and bedside blood tests to distinguish between infection types. Synthesizing these elements seamlessly for an African hospital setting is a complex puzzle, requiring evaluation from collaborating partners in the field. For this reason, further project implementation will account for Malawian partners’ input on hardware durability and software usability. Job remarked that Malawi is an apt setting to pilot this technology, due to it being politically stable and having a health system that has developed significantly over the past few decades. More relevant to this project, however, is that Malawi has limited medical resources, which has impacted its child mortality rates. Child mortality, coupled with an innovative healthcare system, is why Malawi is internationally known as a breeding place for initiatives to improve care for critically ill children. Job would continue this trend by promoting an intervention to prevent deaths amongst children from treatable or preventable complications.
In high-resource settings, monitoring vital signs like heart rate, blood pressure, and respiratory rate is the standard of care to detect these conditions at an early stage. Yet, these monitoring tools are not available in countries like Malawi. Existing monitoring systems are designed for high-income settings and cost a few thousand euros with expensive disposable sensors that require constant repurchasing. These prices exceed the financial capacity of low-resource hospitals and are often complex to use and interpret. These systems can break down or may not be used adequately and thus prove ineffective in low-resource settings. Additionally, the detection mechanisms of these monitoring systems may not be sufficient in wards in Malawi that are often understaffed by nurses, especially at night. This would mean that treatment for otherwise curable complications arrives too late.
For the IMPALA Project, timeliness is of the essence, but only extrinsically so. “I think the main gain is actually patient lives rather than time.” Job asserts that it can decrease the workload of healthcare personnel, but it can also create more labor, as identifying children with critical illnesses will necessitate more action. He explains, “It helps to focus the attention of the limited staff to the ones that really deserve it.” Additionally, early detection of critical illnesses means treatment becomes more feasible, whereas late-stage detection may make proper care a Sisyphean task. Ideally, this monitoring system will not only be able to detect problems as they occur, but also predict them, allowing timely interventions to prevent complications from developing.
A novel feature of the IMPALA system is its clever use of artificial intelligence for detecting developing illnesses. The IMPALA monitoring system, measuring key biomarkers, will compare the data from patients with predictive algorithms created through machine learning. Once integrated, artificial intelligence should be able to predict critical illnesses before they develop. Job notes that data trends from a Dutch hospital setting and an African setting may be different, however. Thus, these predictive algorithms will be developed as part of IMPALA and implemented in the design.
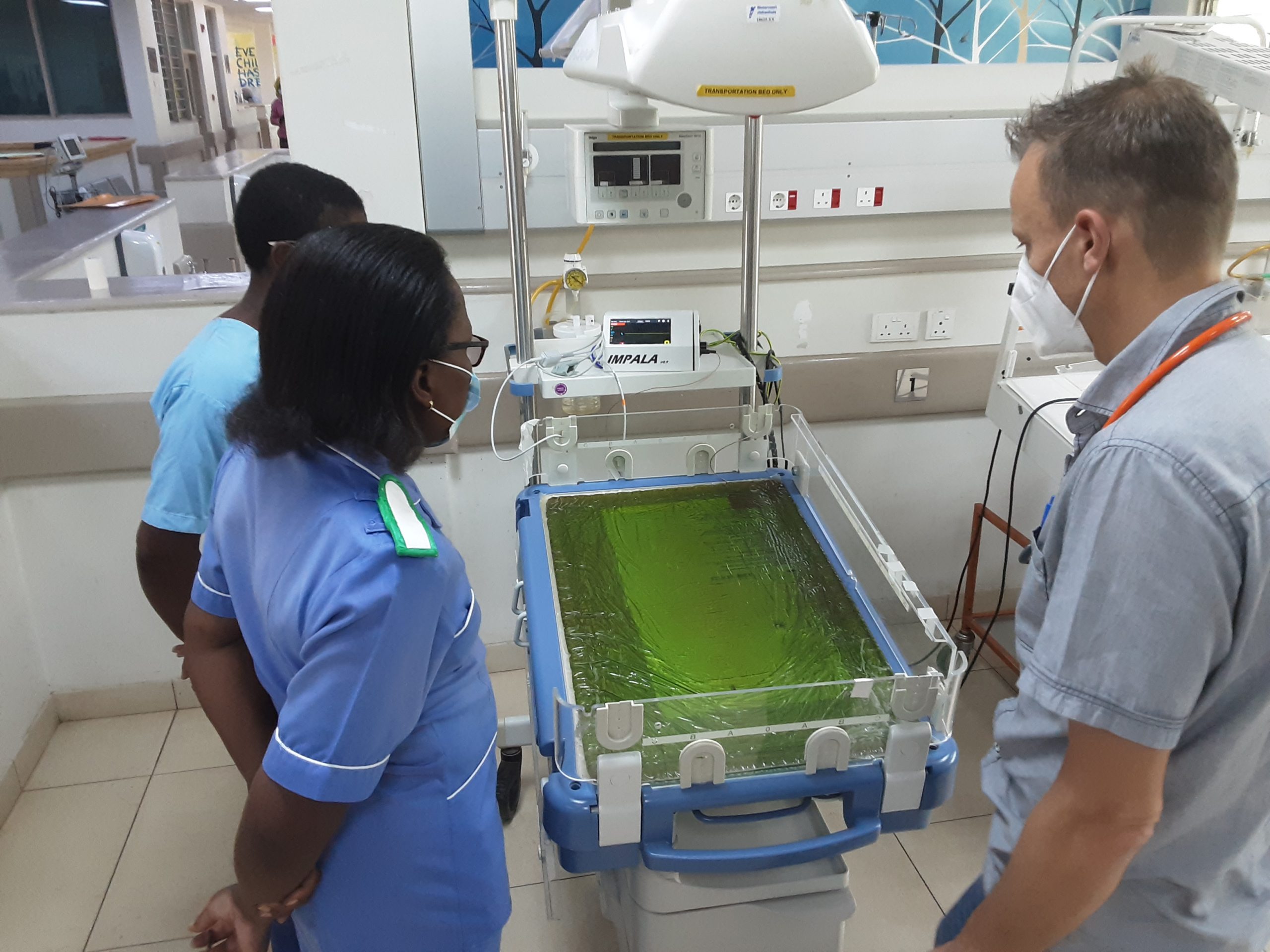
The use of artificial intelligence and machine learning are not the only innovations incorporated into the IMPALA Project. IMPALA monitors circumvent the aforementioned issue of sensors that need to be replaced and manually attached to patients by using a pressure-sensitive, ballistographic mat developed by GOAL 3 that patients lay on to detect vital signs like heart rate, blood pressure and breathe rate. According to Job, this has reduced the possibility of detection error should contact sensors be not properly attached. Additionally, also incorporated into this initiative is novel bedside blood testing, which can not only detect infections, but also distinguish between those that are viral, bacterial and parasitic, circumventing the need for conducting lab tests in low-resource settings. It is cutting edge technology and creative solutions to deficits in medical resources that make the IMPALA monitoring system a radical means of curbing child mortality in low-income countries like Malawi.
Project IMPALA highlights AIGHD’s mission: to provide sustainable solutions to major health problems across our planet by forging synergies between disciplines, health care delivery, research, and education. Project IMPALA demonstrates the importance of collaboration among various disciplines, institutions, and countries. The project builds on strong inter-university connections, as well as the collaboration between researchers in Malawi and Europe.
AIGHD is the coordinating institute for this project and is heavily involved in its implementation. With its multidisciplinary expertise, AIGHD will channel various modes of investigation to assess the implementation of the IMPALA technology. Applying her expertise in development economics, Dr. Wendy Janssens will assess the fiscal feasibility of developing a monitor that costs one dollar per day to operate, while Dr. Christopher Pell will investigate the implementation of this new technology to understand how it can be used by health care workers in Malawi. “AIGHD, being the coordinating institute with experience in large interdisciplinary projects, is essential,” explains Job.
The first pilot study for the prototype IMPALA monitor in Malawi is set to finish by the end of May, for which 50 patients have been recruited. Between various stakeholders and collaborators in this interdisciplinary initiative, including healthcare workers in Malawi, researchers at AIGHD, biomedical engineers at GOAL 3, the department of biomedical engineering at the Malawi University of Business and Applied Sciences, the College of Medicine at Kamuzu University of Health Sciences, the Training Research Unit of Excellence (TRUE) in Malawi, English Imperial College of Science, Technology and Medicine at the Imperial College of London (ICL), the University of Amsterdam, Vrije Universiteit Amsterdam and the Dutch National eHealth Living Lab (NeLL), the future prospects of this monitoring system are bright. Commenting on this larger team effort, Job remarked, “one of the great things about the project is everyone is really enthusiastic about the goal: the development of the monitor. Everybody sees there is a need for it and the potential impact of such a project. Everyone is really motivated. It’s great that we can pull our efforts together and make this work.” We all see it can greatly reduce the number of children dying in hospitals in all low-to-middle income settings. This is a potentially very large number knowing that 90% of all pediatric admissions are in low-income settings and half of them may be preventable.